Growing old brings wisdom, memories, and milestones. But for many elderly patients, it can also bring a silent, life-threatening condition — aortic stenosis.
For decades, severe valve disease meant one thing: open-heart surgery.
But what happens when a patient is too old, too frail, or too medically complex to survive major surgery?
Today, there is hope.
That hope is called TAVR.
Understanding the Problem: Aortic Stenosis
Aortic Stenosis is a condition where the aortic valve becomes thickened and narrowed. This prevents blood from flowing properly from the heart to the body.
Over time, the heart struggles harder and harder to pump blood.
Common Symptoms in Elderly Patients:
-
Breathlessness while walking
-
Chest pain
-
Fatigue
-
Dizziness or fainting
-
Swelling in legs
-
Reduced ability to perform daily activities
In severe cases, untreated aortic stenosis can lead to heart failure and sudden death.
Once symptoms begin, survival without treatment drops dramatically.
And that’s where timing becomes critical.
Why Open-Heart Surgery Isn’t Always an Option
Traditional treatment involved surgical aortic valve replacement (SAVR) — an open-heart procedure requiring:
-
Large chest incision
-
Heart-lung machine
-
General anesthesia
-
Weeks of recovery
For many elderly patients — especially those above 75–80 years — surgery can carry high risks:
-
Weak lungs
-
Kidney dysfunction
-
Diabetes
-
Prior bypass surgery
-
Frailty
-
Stroke risk
In the past, these patients were often told:
“Surgery is too risky.”
But medicine has evolved.
What Is TAVR?
Transcatheter Aortic Valve Replacement (TAVR) is a minimally invasive procedure that replaces the diseased aortic valve without opening the chest.
It is also called TAVI (Transcatheter Aortic Valve Implantation).
Instead of open surgery, doctors insert a new valve through a catheter — usually via a small puncture in the groin artery.
The new valve expands inside the old valve and immediately starts functioning.
No large incision.
No stopping the heart.
No prolonged ICU stay in most cases.
How TAVR Works — Step by Step
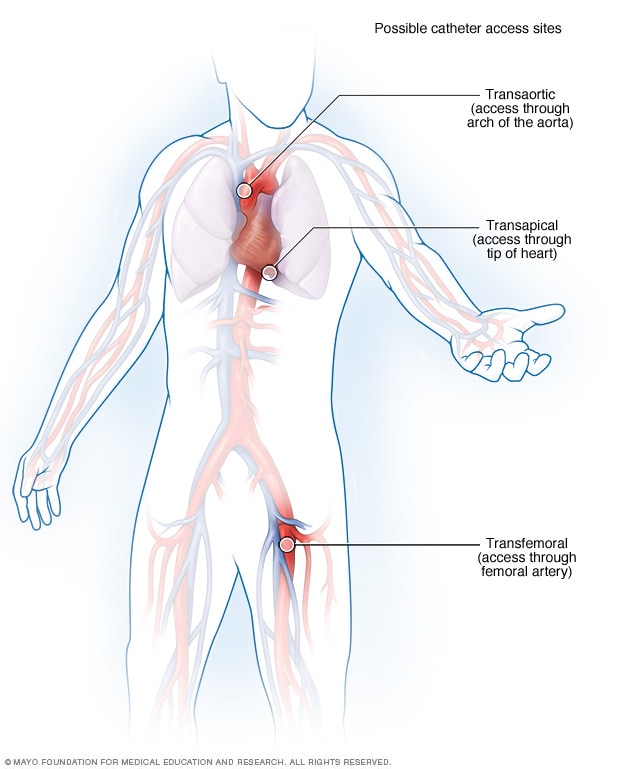


1️⃣ A catheter is inserted through the femoral artery in the groin.
2️⃣ The collapsed artificial valve is guided up to the heart.
3️⃣ It is positioned inside the diseased aortic valve.
4️⃣ The valve is expanded (balloon or self-expanding).
5️⃣ The new valve immediately begins regulating blood flow.
The entire procedure typically takes 1–2 hours.
Many patients are walking the next day.
Who Is Eligible for TAVR?
Initially, TAVR was reserved only for patients considered inoperable.
Today, clinical trials have expanded its use to:
-
High-risk patients
-
Intermediate-risk patients
-
Even selected low-risk elderly patients
Candidates typically include:
✔ Severe symptomatic aortic stenosis
✔ Elderly patients (often above 70–75 years)
✔ Patients with high surgical risk
✔ Patients with previous bypass surgery
A heart team — including cardiologists and cardiac surgeons — evaluates each case.
The Impact: A Second Chance at Life
The transformation can be dramatic.
Patients who:
-
Couldn’t walk across a room
-
Needed oxygen support
-
Experienced frequent fainting
Often report:
-
Improved breathing within days
-
Increased stamina
-
Return to daily activities
-
Better quality of life
For many families, TAVR feels like getting their loved one back.
Why Every Second Counts
Severe aortic stenosis is not just a “valve issue.”
Once symptoms appear:
-
Mortality increases sharply
-
Heart muscle weakens
-
Risk of sudden cardiac death rises
Delaying treatment can permanently damage the heart.
That’s why early diagnosis and timely intervention are critical.
If an elderly patient experiences:
-
Breathlessness on minimal exertion
-
Chest tightness
-
Fainting episodes
It’s important to consult a cardiologist immediately.
Safety and Recovery
Compared to open surgery, TAVR offers:
-
Smaller incision
-
Less blood loss
-
Shorter hospital stay (often 2–3 days)
-
Faster recovery
-
Reduced pain
However, like any procedure, risks exist:
-
Stroke
-
Bleeding
-
Pacemaker requirement
-
Vascular complications
With modern technology and experienced heart teams, complication rates have significantly reduced.
TAVR vs Open Surgery: A Quick Comparison
| Feature | Open Surgery | TAVR |
|---|---|---|
| Chest Opening | Yes | No |
| Heart Stopped | Yes | No |
| ICU Stay | Longer | Shorter |
| Recovery | 4–8 weeks | 1–2 weeks |
| Best For | Younger patients | Elderly/high-risk |
Both procedures have their place. The decision depends on age, risk profile, anatomy, and patient preference.
The Emotional Side of Decision-Making
For elderly patients, fear of surgery is real.
Families often struggle with questions:
-
Is the patient too old?
-
Will recovery be painful?
-
Is it worth the risk?
TAVR has changed that conversation.
Instead of “too risky,” we now ask:
“Is the patient suitable for TAVR?”
It shifts the narrative from limitation to possibility.
Real-World Outcomes
Large global trials have shown:
-
Significant survival benefit
-
Improved quality of life
-
Reduced hospital readmissions
-
Durable valve function over years
For many patients in their 80s and even 90s, TAVR has extended life meaningfully — not just longer, but better.
Frequently Asked Questions (FAQs)
1. Is TAVR safe for patients above 80 years?
Yes. In fact, TAVR was initially developed specifically for elderly high-risk patients.
2. How long does a TAVR valve last?
Current data shows good durability up to 8–10 years and ongoing studies are evaluating longer-term outcomes.
3. Is general anesthesia required?
Many centers perform TAVR under conscious sedation, reducing recovery time.
4. Will I need a pacemaker after TAVR?
Some patients may require a pacemaker. The need depends on individual anatomy and valve type.
5. How soon can normal activity resume?
Light activities often resume within days. Full recovery is much faster compared to open surgery.
6. Does TAVR cure heart failure?
TAVR treats aortic stenosis. If heart failure is caused by valve narrowing, symptoms may improve significantly.
7. Can someone who already had bypass surgery undergo TAVR?
Yes. In fact, TAVR is often preferred in such patients to avoid repeat open surgery.
8. Is TAVR covered by insurance?
In many countries and hospitals, TAVR is covered under major insurance policies. Coverage varies based on plan and region.
Dr. V. Rajasekhar Varada

Senior Interventional Cardiologist & Electrophysiologist
MD, DM (Cardiology)
Clinical Director – Cardiology
📍 Yashoda Hospitals Hitec City
📍 Kothaguda, Hyder
About Dr. Rajasekhar
Dr. V. Rajasekhar Varada is one of the most experienced and highly regarded cardiologists in Hyderabad, with over 27 years of clinical excellence in both Interventional Cardiology and Electrophysiology.
He is uniquely recognized for his dual expertise — performing high-risk complex coronary interventions as well as advanced electrophysiology procedures including catheter ablations and device implantations.
With an impressive annual volume of:
-
~700 Angioplasties
-
~300 Electrophysiology Procedures
-
100+ Device Implantations (CRT, AICD, Leadless Pacemakers)
Dr. Rajasekhar is considered a high-volume operator with advanced technical mastery, particularly in image-guided and complex cardiac interventions.